- Actively manage patients with ≥2 capillary glucose levels >12 mmol/L in 24 hr
- Refer patients with persistent hyperglycaemia (>12 mmol/L), DKA or HHS to diabetes team
- for full list of criteria for referral to diabetes team, see referral to diabetes team guideline
RECOGNITION AND ASSESSMENT
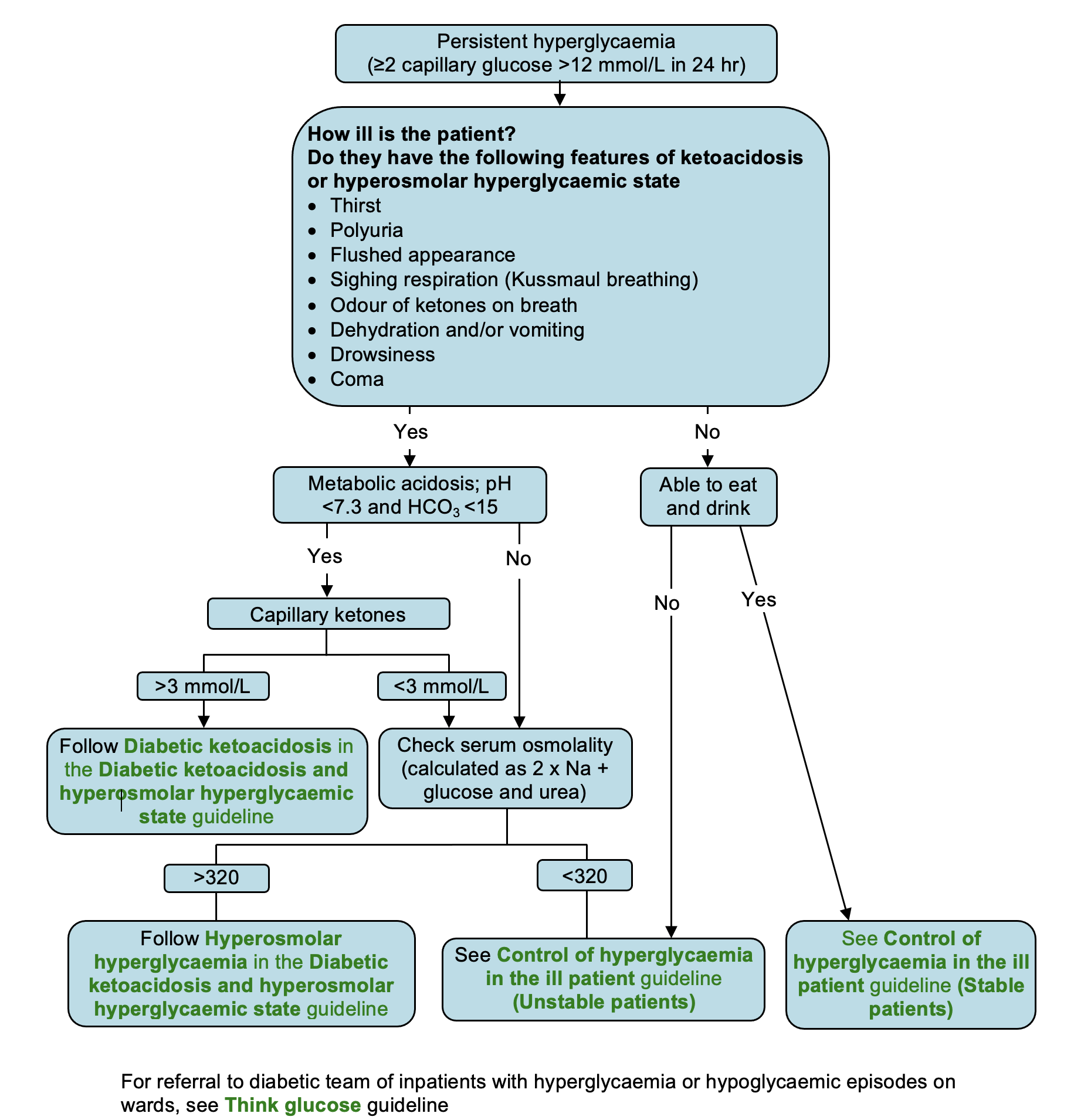
Symptoms and signs suggesting DKA or HHS
- Thirst
- Polyuria
- Flushed appearance
- Hyperventilation (Kussmaul breathing)
- Odour of ketones on breath – not always present or detectable
- Dehydration and/or vomiting
- Drowsiness
- Coma
Investigations for classifying hyperglycaemia
- Blood glucose (capillary)
- Test for ketones in urine
- U&E,
- Blood glucose (venous)
- Venous blood gases
- if SpO2 <94%, arterial blood gas
- If metabolic acidosis present (pH <7.3), check capillary (blood) ketones
- if not available on ward, assume acidosis with high glucose and ketonuria is DKA unless proved otherwise
- even in type 2 diabetes, severe hyperglycaemia can temporarily suppress insulin secretion leading to keto (metabolic) acidosis
- however, in any metabolic acidosis, check for causes other than diabetic ketoacidosis
- Calculate or measure serum osmolality (2 x Na + urea + glucose)
Guidance on severity of hyperglycaemia
(≥2 capillary glucose >12 mmol/L in 24 hr)
© 2022 The Bedside Clinical Guidelines Partnership.
Created by University Hospital North Midlands and Keele University School of Computing and Mathematics.
Research and development team: James Mitchell, Ed de Quincey, Charles Pantin, Naveed Mustfa